By Meghan McCarthy
The connection between mental health and Alzheimer’s disease and related dementias (ADRDs) is often overlooked and understudied. Research shows that individuals with psychiatric conditions such as bipolar disorder or anxiety have a significantly heightened risk of developing ADRDs. Approximately 30 to 50% of Alzheimer’s disease (AD) patients also experience symptoms of depression, and roughly 40% exhibit symptoms of anxiety.
Researchers continue to ask: How do cognitive symptoms of psychiatric illness evolve into AD? And why do some individuals with no prior history of mental illness develop anxiety or depression for the first time after a dementia diagnosis?
Brent Forester, MD, holds multiple leadership roles at Tufts—serving as the Dr. Frances S. Arkin chair and professor of Psychiatry at Tufts University School of Medicine, psychiatrist-in-chief and chair of Psychiatry at Tufts Medical Center, and director of Behavioral Health at Tufts Medicine. Throughout his career, he has focused on the intersection of psychiatric illness and dementia.
“Mental illness and dementia are family issues,” Dr. Forester said. “It touches everyone. I don’t know anyone who doesn’t have these issues in their family. No one escapes this.”

A Personal Connection
As a geriatric psychiatrist, Dr. Forester’s passion stems from personal experience. Both of his physician grandfathers passed away nearly 25 years before his grandmothers.
“As widows, they had enjoyable careers and lives,” he said. “When people think about aging, they often think about it from a negative and ageist mentality. I had a much more positive experience with aging in that way.”
Early in his career, Dr. Forester worked in community mental health centers. He noticed that many older patients with mental health disorders such as depression and anxiety also showed signs of cognitive decline—yet often went undiagnosed for ADRD.
“There was a lack of awareness in the field of mental health about the complex interaction between people aging with mental illness and those people with cognitive issues,” Dr. Forester said.
This realization prompted Dr. Forester to focus on the biological mechanisms that influence medication response in individuals with bipolar disorder. This led him to a deeper interest in studying bipolar disorder, specifically in older adults.
Understanding the Link
Bipolar disorder is a psychiatric condition that affects an individual’s energy levels, mood, and focus. It is marked by mood episodes—either manic, depressive, or mixed. Mania may include symptoms such as racing thoughts and euphoria, while mixed episodes feature symptoms of both depression and mania. Among psychiatric conditions, mania is the most heritable.
A diagnosis of bipolar disorder requires a patient to experience at least one episode of mania in their lifetime. While the exact percentage is unknown, clinicians widely agree that individuals with bipolar disorder are at increased risk for developing ADRDs.
Cognitive symptoms, including executive dysfunction, memory retrieval issues, and attention difficulties, are core features of bipolar disorder. While these symptoms intensify during manic episodes, they often persist at a lower level throughout a person’s life.
“We have found that there seems to be a decline in cognition as people age with this illness,” he said. “The question is: Is that a new neurodegenerative illness, like AD, or is it the course of bipolar disorder?”

Understanding Bipolar Disorder in Older Adults
Bipolar disorder can appear in adolescence, adulthood, or later in life. But much of psychiatric research has focused on younger populations, leaving gaps in understanding its trajectory in older adults.
To address this, the Global Aging and Geriatric Experiments in Bipolar Disorder (GAGE-BD) developed a data-sharing initiative to analyze previously collected information from individuals with bipolar disorder. This project aims to provide insights into the illness trajectory, cognitive decline, biomarkers, and neuroimaging findings in older adults with bipolar disorder (OABD).
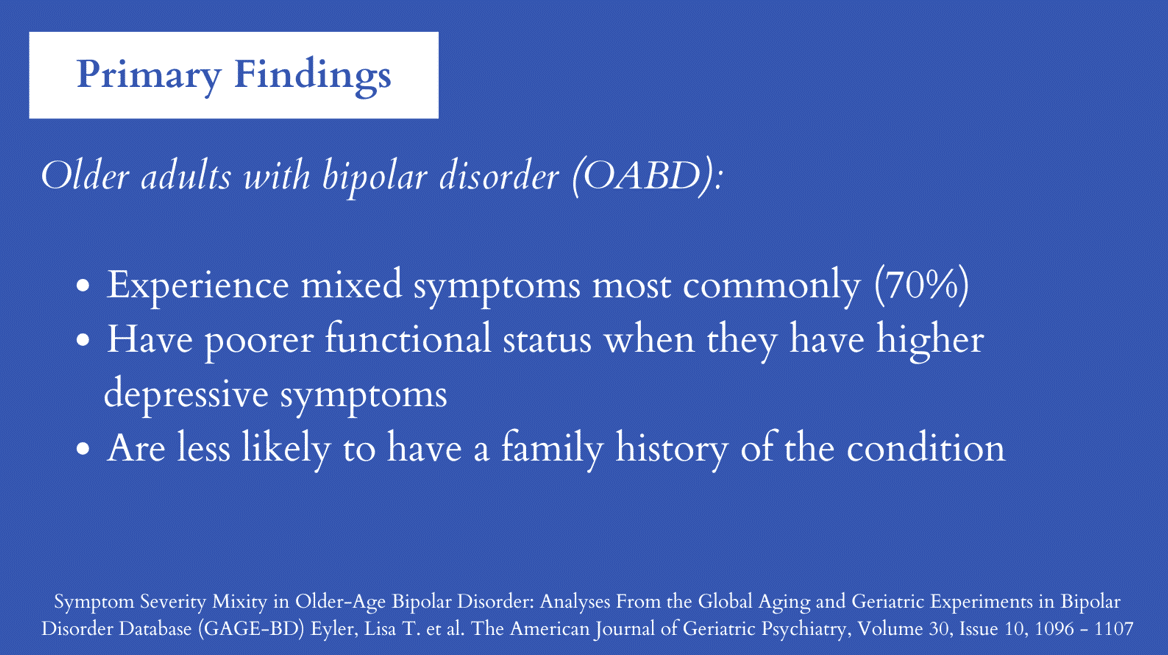
Dr. Forester and his team have explored how different characteristics and symptoms vary based on the age of bipolar onset. Their research found that nearly 70% of OABD patients experience mixed symptoms, a presentation less common in younger individuals. Instead of experiencing euphoric mania, older adults are more likely to have mixed manic and depressive symptoms.
Additionally, OABD patients who experience mixed symptoms, particularly those in which depression is more prominent, often have the poorest functioning. These findings suggest that treatments targeting bipolar depression may be most effective in managing OABD.
Another key distinction is that older adults with bipolar disorder are less likely to have a family history of the condition. Instead, late-onset bipolar disorder is often triggered by underlying medical or neurological issues or as a side effect of medication.
Scaling Mental Health Care for Aging Populations
While the exact relationship between neurodegenerative and psychiatric illnesses requires further research, projects like GAGE-BD are helping bridge knowledge gaps.
“Clinical trials and research are a way for someone who is a clinician and educator at heart to address unanswered questions,” Dr. Forester said. “Research is also a way to create interprofessional balance. It sets time aside to think and be innovative.”
Beyond individual psychiatric disorders, Dr. Forester’s work emphasizes public health strategies to improve geriatric mental health care. His goal is to create standardized protocols and programs that can be implemented in primary care settings to better support patients with dementia and psychiatric conditions.
“The public health approach is so critical to geriatric mental health,” he said. “I want to find a way to do dementia care in primary care. How do we bring the gold standard for assessments, diagnostics, support for the family, and interventions with patients and scale it for primary care?”
To learn more about Dr. Forester, please click here.
To read Dr. Forester’s book, The Complete Family Guide to Dementia, please click here.
To read, Bipolar Disorder in Older Adult Patients, which Dr. Forester co-edited, please click here.
To read more about Symptom Severity Mixity in Older-Age Bipolar Disorder, please click here.